Hoof care in foals. Promoting correct conformation for the future equine athlete. |
||||
SummaryThe high monetary and effective investment that the foal represents at birth warrants regular farriery assistance in order to ensure that it develops into a healthy adult performance horse. Regular hoof care enables development problems to be monitored in the early stages when treatment is most effective and has the added advantage of educating young stock to be handled by the farrier. A regular hoof care programme for foals should begin with observation at birth and continue with regular trimming at least every 4 weeks. The subcoronary sulcus, which is present after birth, may require special attention when it approaches the distal border of the hoof at the age of 2-3 months. The evaluation of conformation in foals should be prudent, as base-wide and toe-out stances can be considered normal in most cases and therefore should not be corrected. Conversely, orthopaedic correction is necessary in the case of flexor-flaccidity, flexor-contraction and angular deviations. The latter may require a combination of surgical and orthopaedic farriery techniques. Correction in young foals can be achieved through trimming, glue-on shoes, extensions with acrylics or a combination of these with aluminium plates. Other problems that may need therapy are excessive wear, cracks, hoof wall defects, white-line disease and solar abscesses. Keeping a written and / or photographic record of the foals in one's care can be useful to assessing progress of the individual and to detecting genetic transmission of certain defects and is usually appreciated by the breeder. |
||||
IntroductionThe new-born foal generally represents an important economic, and often also effective, investment and it therefore makes sense to promote all of the environmental factors that will assist the foal in its harmonious development into an adult performance horse that is able to express its genetic potential. Regular farriery, and in broader terms, podiatry care are doubtless of primary importance in the prevention and correction of defective limb conformation. |
||||
Regular careThere are two practical reasons for giving regular farriery/podiatry assistance to foals:
|
||||
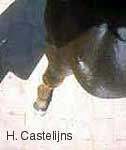
Special characteristics of foalsAt birth the foal's hoofs are enveloped in the perioplic membrane, which reduces the risks to the mare's birth channel. With the first steps the perioplic membrane on the solar surface wears and retracts proximally on the hoof wall where, drying out, it tends to create a sulcus of varying depth below the coronary band. This depression, which is to be considered normal, may, however, cause irregular wear of the hoof's ground surface when it grows down towards the age of three months. |
||||
|
||||
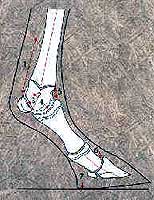
Due to its growth the foal presents a dynamic, constantly evolving model and therefore its conformation cannot be judged in the way an adult horse is appraised. In precocious, dolicomorphic breeds, for example, the narrow chest together with the relatively long limbs cause many foals to adopt a slightly base-wide stance in front (often accompanied by outward rotation of the entire limb). This stance, which is to be considered as quite normal in young subjects, confers a higher degree of stability and is gradually modified as the transverse diameters of the upper body increase with growth. A base-wide stance in a 3- to 4-month-old foal results naturally in slightly asymmetric hoof capsules in the frontal plane (latero-medial), with the medial side of the hoof capsule of each limb slightly lower then the lateral aspect; if this stance is not recognised as physiological for this age and type of foal and an attempt in made to "correct", by lowering the lateral hoof walls, or through medial extensions, there is a risk of creating an angular deviation (A.D) (e.g. a varus fetlock) where none existed previously. The aim of farriery treatment should be the prevention or correction of true A.D.s and rotations present within the limb by maintaining or re-establishing the alignment of its different bony segments. A useful observation to evaluate this alignment is obtained by looking down at the entire limb from a position close to the subject. |
||||
|
||||
Flexor flaccidityFlexor flaccidity is usually a defect of the new-born that affects both hind limbs. It has been described as a defect that tends to self-correct within days with moderate exercise without the need for treatment. |
||||
|
||||
It is, however, the author's experience that is not that rare to observe 4- to 6-week-olds who are still lifting the toes off the ground when loading the limb. The possible consequences of the hyperextension of the distal interphalangeal (D.I.P.) joint, which accompanies flexor flaccidity include: i) inflammation of the suspensory ligament, ii) instability of the distal metatarsal III epiphysis, iii) remodelling of the distal articular cartilage of the metatarsus III in the area where it contacts the proximal sesamoids, iv) and the first phalanx, v) remodelling and osteochondral fragmentation of the dorsal articular margins of the metatarsal-phalangeal joint, vi) remodelling and parcelar fragmentation (chips) of the dorsal articular margins of the third phalanx (P3), vii) crushed and excessively worn heels with ulceration of the bulbs, viii) inflammation of the plantar ligament and curb. |
||||
|
||||
A plantar extension, which reaches about 3-4 cm behind the bulbs, immediately relieves the biomechanical instability. In order to apply the extension it is useful to work on the foal in decubitus on a thick layer of bedding, thereby preventing weight bearing on the extension before the glue or resin has cured sufficiently to assure a resistant bond. It is important to assure the correct alignment of the extension with the foot. In the new-born or in days-old foals there is no need for sedation if qualified help is available; the presence of the mare, held by an assistant, tranquillises the foal. In the days-old foal, the time during which it carries cuff-type extension shoes should not exceed 10-12 days, so as to limit the constriction of the hoof caused by the cuff. As an alternative to the cuff shoes, small aluminium plate extensions with clips can be applied to the hoof with methacrylate resins. Moderate exercise on compact surfaces and minimum bedding depth are to be recommended. Recidivity is rare and is usually only seen in those cases where the extensions were applied rather late (after 3-4 weeks of age). |
||||
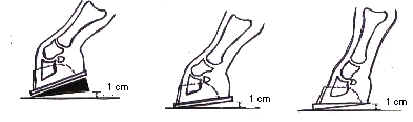
Flexor contracturesFlexor contractures may involve the deep digital flexor (DDF) tendon and muscle unit, the superficial digital flexor (SDF) tendon and muscle or both. The DDF tendon attaches to P3 at the semilunar line, P3 being attached to the hoof capsule, dorsal extensions are indicated for the treatment of DDF tendon/muscle contractures. A pain-contracture-pain-further contraction vicious circle seems to play a central role in flexor contractures and simply lowering the heels may cause an aggravation of pain in severe contracture cases. The Dallmer ® (club foot) glue-on shoes are supplied with a screw-on heel wedge, which can be progressively rasped down after raising the heels initially. The imprint the heels leave on the ground can be used as the sign to reduce the height of the wedge until, after removing it completely, the phalangeal axis can be further aligned by the use of the Dallmer ® BK model, which has a slight toe wedge. The Ibex ® cuff glue-on system also has wedges available, which may be glued on under the shoes. |
||||
|
||||
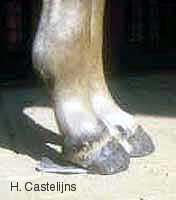
Applying cuff type glue-on shoes with heel wedges is best done on the standing, sedated foal, the dorsal hoof wall being pressed into close contact with the rim of the cuff by the action of the heel wedge. Care must be taken that there is no rotation of the limb during the time the glue is still fluid as this causes a misalignment between the sagittal axes of the shoe and the hoof. Synthetic floors should be avoided, as there is a risk of glueing the foal to the ground! For a favourable prognosis it is important to act early at the first signs of contracture, combining the dorsal extensions with appropriate medical treatment (e.g. analgesics, tetracyclines) and dietary restriction. The so-called "grass foot" syndrome, consisting of the development of an upright narrow hoof on one forelimb with the controlateral hoof being flat and low-heeled is often due to the stance some short-necked, long-limbed foals assume to get at the pasture. One foot will be placed forward (overloading the heels) and the other under the body (loading the toe). Typically, this can be observed towards 3-4 months of age during growth spurts. |
||||
|
||||
The musculo-tendinous units, including the check ligaments, rapidly adapt to this stance, which sometimes makes it difficult to re-establish a correct phalangeal alignment by conservative means (trimming down the heels, dorsal extensions, toe-tips). Refractionary cases can be recognised by the development of a concave dorsal hoof wall with the growth rings widely divergent at the heels and are candidates for carpal check ligament desmotomy, preferably before the distal interphalangeal joint capsule and articular surfaces are affected. The desmotomy should be accompanied by a rather large dorsal extension, which not only helps to realign the phalangeal axis but also keeps the resected ends of the carpal check ligament distantiated. |
||||
|
||||
For the treatment of SDF tendon-muscular contractures, which bring about the straightening of the pastern with flexion of the fetlock joint ("knuckling"), glue-on shoes can be useful elements for anchoring aluminium splints, which bandaged to the limb, attempt to extend the fetlock joint. SDF contractures are most often observed in 8- to 14-month-olds and have a much poorer prognosis than DDF contractures. Heel elevation, which promotes fetlock extension and radial check ligament desmotomy, may bring about some improvement. |
||||
Angular deviationsCongenital as well as acquired A.D.s are frequent in foals, with the highest incidence at the carpus [6, 9, 10] A.D.s are defined as valgus when there is a lateral deviation of the limb portion below the point of origin and as varus when the deviation of the distal segment is medial. When the angle between the radius and the metacarpus is < 180° on the lateral (concave) side the carpus is defined as valgus and as varus when the angle is > 180° on the lateral (convex) side. As discussed previously, it is important to distinguish between A.D.s and base-wide/outward rotated limbs. In the latter there are no misalignments between the bony segments within the limb. This stance and transitional conformation can be considered normal in dolicomorphic foals and even yearlings, with a tendency to change naturally as growth and development of the circumference of the thorax takes place. Clinical evaluation of A.D.s and of their point of origin are facilitated by observing the limb downwards standing close to the subject's shoulder. |
||||
|
||||
An objective evaluation of the degree of A.D. and of the site where it originates requires a radiographic examination, which is also useful to establish or exclude incomplete ossification of carpal or tarsal bones or Salter-Harris type fractures as cause(s) of the A.D. The chronology of growth plate (G.P.) activity and closure of the different bony segments, particularly of the distal G.P. of the radius (22-42 months), distal G.P. of the metacarpus-tarsus III (6-18 months) and proximal G.P. of the first phalanx (6-15 months) is important for the therapeutic approach, particularly given that the actual times of high growth activity are much more limited. McIlwraith considers the useful times for the correction of A.D.s as the first 3 months for fetlock deviations (distal G.P. of metacarpus-tarsus III, proximal G.P. of the proximal phalanx) and the first 6 months for deviations at the carpus-tarsus (distal G.P. of the radius-tibia). In the latter case, times are not only limited by G.P. closure, which actually happens much later, but also by the risk of precocious insurgence of osteoarticular lesions when the foal acquires body mass. A lateral or medial extension applied to the hoof at an early age (when it is most effective) acts not only on the proximal G.P.s but also on the distal ones. For example, the application of a medial extension, at two months of age for the correction of a carpus valgus might well cause a fetlock varus. It is therefore advisable to combine farriery with surgery such as periostal stripping at the appropriate G.P. when dealing with severe proximal A.D.s (distal G.P. of the radius-tibia) Lateral and medial extensions can be obtained using Dallmer ®, Mustad ® or Ibex ® glue-on shoes or with custom-made aluminium plates fixed to the hoof with methacrylates, as the foal's hoof walls are usually too thin to bear safe nailing. Ideally, the extension should reach sideways to the vertical projection of the convex side of the deviated joint. With a wide extension it is advisable to apply a smooth slope of acrylic to reduce the risk of the foal or the mare pulling it off when accidentally stepping on the extension. |
||||
|
||||
Glue-on extensions are very versatile and can also be used in the correction of rotational defects by cutting the base plate appropriately (extension of the underdeveloped quarter-toe area) or by twisting the glue-on shoe slightly when fixing it to the hoof. Since cuff-type glue-on shoes should not be left on for more then 15-20 days, depending on the age of the foal (the fast-growing hoof risks constriction), severe A.D.s may need repeated applications of extensions (and more then one periostal stripping). It is important to check each time that no "compensatory" counter deviations or rotations are being created distally to the original deviation. Glue-on extensions, when used appropriately, give excellent results both aesthetically and functionally. The therapy for A.D. must further include exercise limitation to prevent excessive compression and concussion on the asymmetrical G.P.s and joints (confinement to the box or to a small pre-paddock). |
||||
Record keepingRecorded notes and/or images of the conformation of foals are useful for the next visit to the stud, permitting a more objective evaluation of positive or negative changes. Historical records containing data from several years can sometimes yield interesting information on the reproductive value of a particular mare or stallion. There is current research work being done to establish objective written and photographic protocols for the evaluation of conformation in foals. |
||||
ConclusionGlue-on shoes for foals have proved to be extremely useful in the treatment of flexor and angular deformities and similar results can also be obtained with the use of aluminium plates fixed with acrylics. The therapy of conformation defects in foals requires a rather large investment in time, material and labour, investment which is amply justified by the achievable results and the potential capital which many foals represent. McKinnon mentions an efficiency index of thoroughbred breeding in the U.K. (offspring that reach the racetrack / mares sent to stud 3 years previously) of only 14% [12]. In other words, the functional recovery of a single foal in a farm of 100 mares would increase productivity by 7%! |









Hans Castelijns
D.V.M - Certified Farrier